
Third Wave (2014 – 2019)

We began the third wave of the SABRE study when participants were entering older age (77 years on average in 2016). Healthy ageing depends on many things, but the function of the heart and brain may be particularly important. Yet information on ethnic and gender differences in heart and brain function are limited and contradictory.
In the third wave we set out to answer some specific questions
- Would heart and brain structure and function be poorer in people from ethnic minority groups than in Europeans? And if so, would any differences be explained by the excess burden of diabetes, its associated adverse metabolic and haemodynamic effects, alone or in combination with high blood pressure?
- Would risk factors measured in mid-life (First Wave 1988-91) add to, or even be better predictors of ill-health in older age than the same risk factors measured in 2008-11?
- Would there be differences between men and women in heart, brain and physical function? And would any difference be the same in all ethnic groups? And would any differences be explained by diabetes?
- Would rates of strokes be higher in ethnic minorities and would this be explained by adverse effects of diabetes and high blood pressure?
- What aspects of health and lifestyle at earlier waves of the study would be associated with healthy ageing?
What did we do at visit 3?
We invited our original study participants to take part in the third wave of the study, together with their partners and some new participants of African and African Caribbean ethnicity.
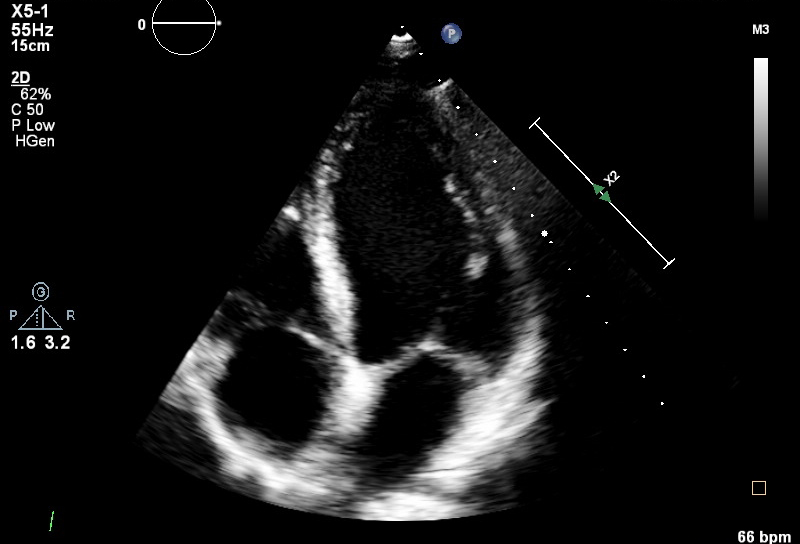
Participants were asked to complete questionnaires about their health and lifestyle and they were invited to attend the study clinic at UCL where they underwent a range of clinical measurements. These included echocardiography, MRI scans of the brain, lung function, cognitive(brain) function, depression, bone density (DEXA scans), various measures of fat and lean mass, exercise capacity, physical activity monitoring, bloods, behavioural and lifestyle factors. We also asked participants for consent for the study to receive data regarding their hospital admissions.
What have we found so far?
We are still analysing much of the very detailed data collected at wave 3, but here is a taste of what we have found so far.
- Encouragingly, we saw relative improvements in survival for both ethnic minority groups over time. We also found that risk factors which were measured at the first wave of SABRE largely explained the higher rates of cardiovascular disease in South Asians across 30 years of follow-up. This suggests that better prevention and treatment could reduce the risk of heart disease and stroke in South Asian people.
- Exercise capacity and muscle function were poorer in South Asian people than in European participants and this may be an important part of the reason why some ethnic minority groups have a greater burden of ill-health in later life. Further research is needed to understand the reasons for this in order that we may develop better preventive measures.
- Studies using MRI of the brain showed that measures of brain blood flow may be more useful as a diagnostic tool in people with advanced dementia than in people with little measurable sign of cognitive impairment. SABRE images have been used to develop a new method of mapping subtle damage to the brain (white matter lesions) and study of these lesions shows that they are related to diastolic blood pressure, particularly in South Asians. This fits with our earlier findings in 2008- 11 that there were stronger links between diastolic blood pressure and stroke in South Asians than in Europeans. This could mean that South Asian people are more susceptible to disease of small blood vessels in the brain compared with Europeans. We also showed that calculations of brain blood flow in some people need to be adjusted for haematocrit levels (the proportion of blood volume that is made up of red blood cells) – this is important for women, people with diabetes and non-European ethnic groups.
- Bone fractures are increasingly important in an ageing population and there are known ethnic differences in bone mineral density, although the reasons for this are unclear- we studied whether body fat distribution or markers if inflammation might explain these ethnic differences. They did not do so- leaving us to consider further research on the links between cardiometabolic and bone health.
- With participants permission we have also shared unidentifiable (anonymised) data with other research groups, so that different academic teams with new ideas may explore and add to the benefits of the research. This data sharing includes SABRE study participation in the Dementias Platform UK, COMETS(Consortium of METabolomics Studies), the UK LLC (Longitudinal Linkage Collaboration), Meta VCI Map population based project (focussing on mapping WMH and examining associations with cognitive decline in non-demented community dwelling individuals). Strong links have been established with CLS (Centre for Longitudinal studies at UCL)